When thinking about the right scoliosis treatment there are many options to consider. This is what you would expect since scoliosis itself is a complex and often highly variable condition which requires a treatment plan specifically designed for each patient.
The two main approaches used in non-surgical scoliosis treatment are scoliosis specific exercise methodologies and bracing. Of the two, bracing is probably the more effective, although a scoliosis specific exercise program can sometimes be sufficient. In some instances, patients might prefer bracing over exercise due to the improved results which can be obtained without conscious efforts.
At the UK Scoliosis clinic, we often use both approaches to achieve the best possible outcome for patients – but today let’s consider bracing.
Why is bracing so popular?
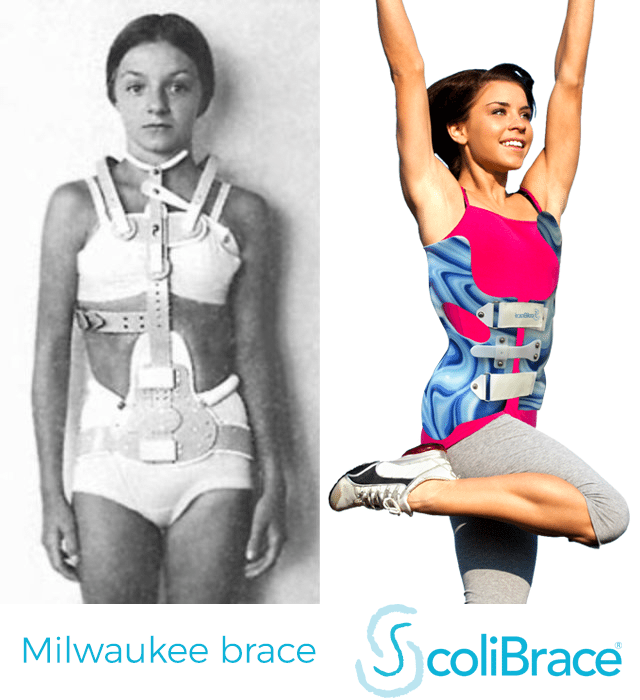
Today, scoliosis patients can benefit from the latest and most technologically advanced braces available through our clinic. Unlike some older brace designs, modern braces present a high likelihood of a successful non-surgical outcome.
To take just a few points, recent research has shown that…
- Specialised scoliosis bracing when prescribed for high-risk patients, can prevent the need for surgery in most cases[1]
- Patients who wear scoliosis braces get better results the longer they wear the brace each day[2]
- Part-time bracing in adults significantly reduces progression of curvatures and improves quality of life[3]
- Conservative treatment with a brace is highly effective in treating juvenile idiopathic scoliosis, with most patients reaching a complete curve correction[4]
- Bracing is an effective treatment method for AIS cases, characterized by positive long-term outcomes[5]
Today, research is therefore clear – scoliosis bracing is an effective, affordable and safe alternative to surgery. But which brace should you choose? With the growth in interest in non-surgical scoliosis treatment, various brace designs have become popular – while each have their own benefits, here at the UK Scoliosis Clinic, we offer the ScoliBrace active correction brace – which we believe to be the most modern an effective brace on the market. Let’s see why:
Why choose ScoliBrace?

ScoliBrace is comfortable, low profile and easy to use!
When choosing a new treatment option for our clinic, our scoliosis specialists scrutinise each aspect of a candidate product, both from a clinical and patient comfort perspective. To date, ScoliBrace is (in our opinion) the best scoliosis braces we have seen, that’s why it’s our go-to treatment in many cases. Originally developed in Australia we are one of only a handful of internationally approved ScoliBrace providers.
ScoliBrace improves upon many previous braces, and avoids some of the most common pitfalls – it is:
Highly effective
A ScoliBrace is an over-corrective brace – unlike braces which simply try to halt the progression of scoliosis, ScoliBrace works by guiding the body and spine into a posture that is the opposite of how the scoliosis is shaped. This means that all the time you are wearing a ScoliBrace, you are treating your scoliosis – not just slowing it down. A ScoliBrace can also help to improve the overall appearance of the body.
Comfortable
Most Scoliosis braces are quite tricky to get into and can sometimes have a less than optimal construction for your body shape. ScoliBrace opens and closes at the front making it easy to wear and remove without assistance. Thanks to our advanced manufacturing process, your brace will be custom made to fit you like a glove.
Stylish
Unlike most braces which are only available in white, ScoliBrace is available in a variety of colours and patterns which allow you to personalise the look of your brace. We can offer exciting patterns for younger children (featuring everything from dinosaurs to football, and butterflies to love hearts) as well as stylised looks from a Demin pattern to Zebra print! ScoliBrace is also available in a wide variety of natural skin tones, to match your own completion if you prefer.
Adjustable
Many scoliosis braces are manufactured to a single size and shape, meaning that over the course of treatment some patients may require three or even four individual braces. ScoliBrace has a wide range of adjustment, meaning that in most cases patients require no more than two braces during treatment – which can save a great deal of money in the long term.
Low profile
ScoliBrace has been designed with everyday people living everyday lives in mind – this means the brace is as unobtrusive as possible and can even be worn during sports and other physical activities. ScoliBrace is intentionally low profile, so that it can be worn almost invisibly under even light clothing.
Totally customised
Many scoliosis braces today claim to be a custom design – but ScoliBrace braces take this principle a step further. ScoliBrace braces are planned out using brace Scan technology, which combines 3D full-body laser scanning, x-rays and posture photographs. Each brace is then custom designed for the individual with Computer Aided design (CAD) and then created with Computer Aided Manufacture (CAM) to create a brace which is perfect both in terms of fit and correction. Thanks to this process our measuring and manufacturing tolerances are as low as 0.5mm.
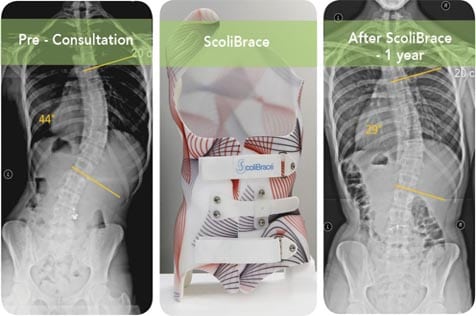
Modern scoliosis braces like ScoliBrace are highly effective
[1] ‘Idiopathic scoliosis patients with curves more than 45 Cobb degrees refusing surgery can be effectively treated through bracing with curve improvements’
Negrini S, Negrini F, and Zaina F, 2011, Spine J. 2011 May;11(5):369-80. doi: 10.1016/j.spinee.2010.12.001. Epub 2011 Feb 2.
‘Effects of Bracing in Adolescents with Idiopathic Scoliosis’ [Results of the BrAIST Clinical Trial]
Stuart L. Weinstein, Lori A. Dolan, James G. Wright, and Matthew B. Dobbs, N Engl J Med 2013; 369:1512-1521 October 17, 2013DOI: 10.1056/NEJMoa1307337
[2] ‘Effects of Bracing in Adolescents with Idiopathic Scoliosis’
Stuart L. Weinstein, Lori A. Dolan, James G. Wright, and Matthew B. Dobbs, N Engl J Med 2013; 369:1512-1521 October 17, 2013DOI: 10.1056/NEJMoa1307337
[3] ‘Effects of Bracing in Adult With Scoliosis: A Retrospective Study‘
Palazzo C, Montigny JP, Barbot F, Bussel B, Vaugier I, Fort D, Courtois I, Marty-Poumarat C, Arch Phys Med Rehabil. 2016 Jun 22. pii: S0003-9993(16)30256-8. doi: 10.1016/j.apmr.2016.05.019
[4] ‘Brace treatment in juvenile idiopathic scoliosis: a prospective study in accordance with the SRS criteria for bracing studies – SOSORT award 2013 winner‘
Angelo G Aulisa, Vincenzo Guzzanti, Emanuele Marzetti,Marco Giordano, Francesco Falciglia and Lorenzo Aulisa, Scoliosis 2014 9:3 DOI: 10.1186/1748-7161-9-3
[5] Curve progression after long-term brace treatment in adolescent idiopathic scoliosis: comparative results between over and under 30 Cobb degrees
Aulisa et al, Scoliosis and Spinal Disorders 2017 12:36 https://doi.org/10.1186/s13013-017-0142-y