At the UK Scoliosis clinic, our primary focus is to allow as many patients as possible to benefit from the chance to beat scoliosis through non-surgical methods as possible. Research as well as our own experience demonstrates that scoliosis bracing is the best way to achieve this – and for this reason were broadly supportive of any kind of scoliosis bracing technology available. This being said, we’ve said before that all braces are not created equal – some are just more effective than others.
Why ScoliBrace?
Our preferred brace and the one we offer at the clinic is the ScoliBrace. ScoliBrace is a totally customised brace, designed to achieve maximum curve correction as quickly as possible – but as well as being a highly effective corrective device, ScoliBrace is (in our opinion) the most patient-friendly brace on the market. It’s a low profile brace, and is practically invisible under clothing – unlike traditional braces, ScoliBrace opens and closes at the front making it easy to wear and remove without assistance. ScoliBrace is even flexible enough to allow the wearer to participate in normal physical activity while wearing the brace. What’s more, you can customise your ScoliBrace! – There are a variety of colours and patterns available for patients to personalise the look of their brace – overall, we think these factors make it the best choice for patients today.
How effective is ScoliBrace?
ScoliBrace stacks up favourably vs. the traditional thoracolumbosacral orthosis (TLSO) braces available through hospitals and some other clinics – and one recent study shows just how great the difference can be. The recently published study from Dr Jeb McAviney of ScoliCare (Sydney, Australia) concerned a male patient who was referred to the ScoliCare clinic at the age of seven with a previous diagnosis of juvenile idiopathic scoliosis. The patient had previously been fitted with a traditional 3-point pressure thoraco-lumbo-sacral orthosis (TLSO) that had been designed by a hospital orthotist[1].
The patient reported that he regularly participated in rugby, soccer and swimming. Aside from the spinal deformity, the patient was otherwise healthy. On examination a right thoracic curve and a left lumbar curve were noted.
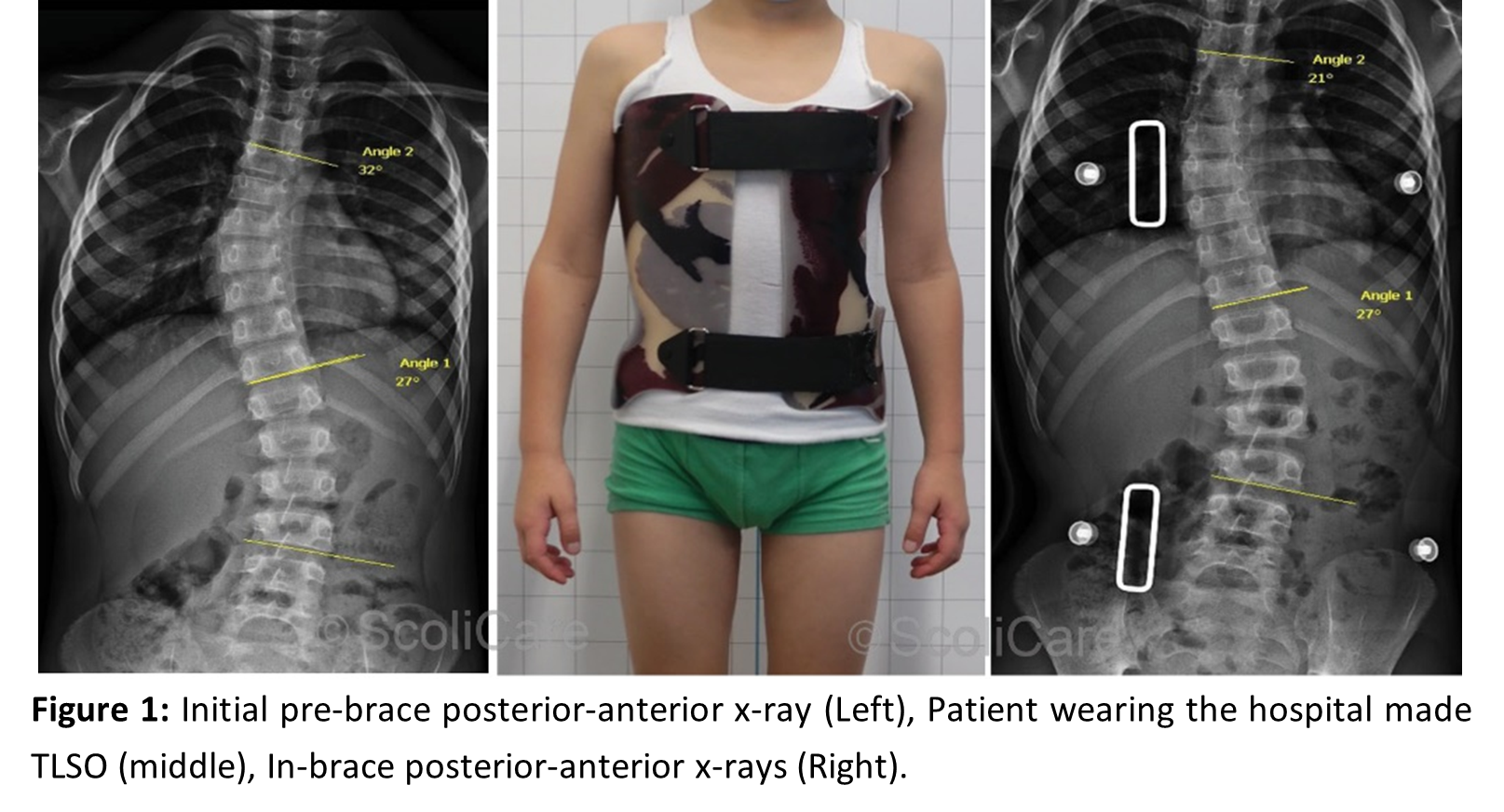
The patient provided x-rays that had been taken at the time of the initial diagnosis as well as x-rays taken soon after the brace fitting (Figure 1). The initial pre-brace x-rays revealed that the patient’s primary thoracic curve was 32° Cobb and the secondary lumbar curve was 27° Cobb.
An examination of the in-brace x-rays for the hospital made TLSO demonstrated that an adequate in-brace correction had not been achieved with only an 11° reduction in the thoracic curve and no measurable change in the magnitude of the lumbar curve (Figure 1).
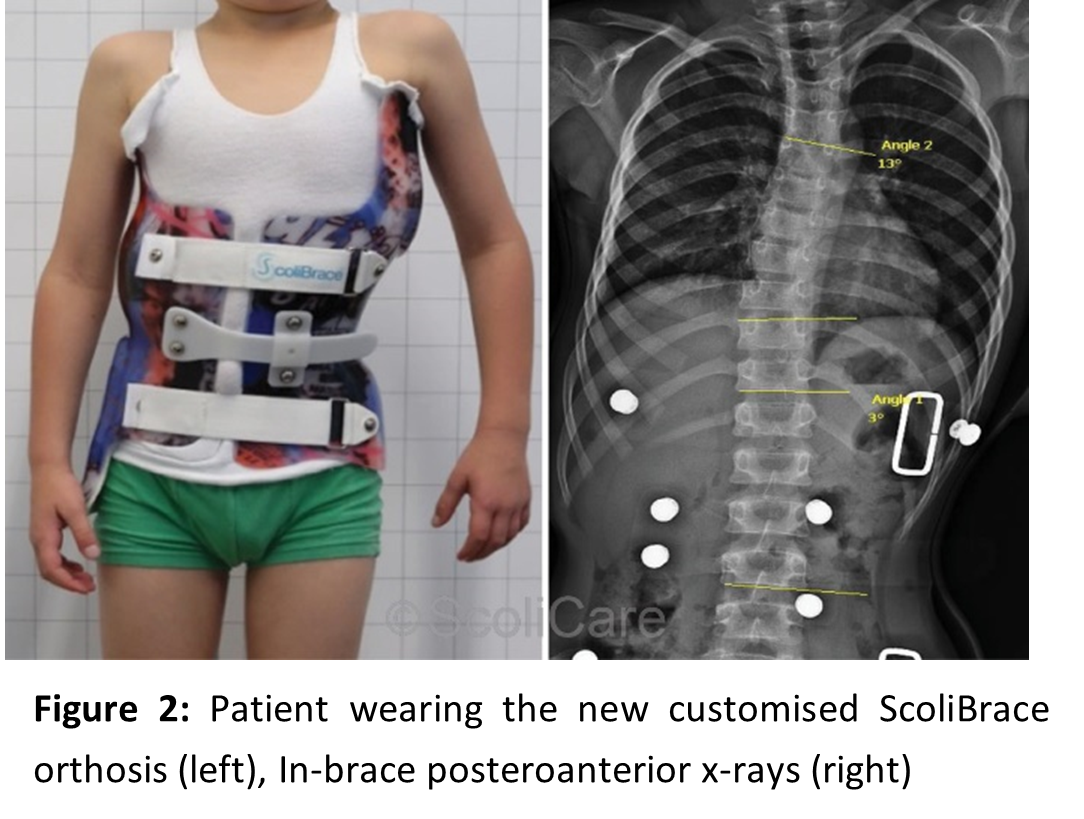
Dr McAviney proceeded to design and fit a customised ScoliBrace for the patient – In-brace x-rays taken soon after the fitting of the new ScoliBrace demonstrated a significantly better in-brace correction compared to the previous brace.
The patient’s primary thoracic curve had been reduced to down to 13° Cobb, which represented a 59% correction of the initial curve and a 25% improvement on the correction obtained with the hospital-made TLSO.
The lumbar scoliosis was almost completely reduced (3° Cobb) in the new orthosis. The hospital-made TLSO had not achieved any correction in this region of the spine (Figure 2).
This is just one case which demonstrates that all braces are not equal – the right brace at the right time is needed for real improvement.
Is ScoliBrace right for me?
If you’ve been diagnosed with scoliosis you will have numerous treatment options – bracing is one of these, while exercise-based therapy is the other major one. For very small curves exercise-based approaches may be preferable, but in most cases, we recommend you consider bracing.
Since Scoliosis presents in a unique way in every patient, ScoliBraces are custom designed to fit your exact needs – Fundamentally, Scoliosis is a 3 Dimensional condition, so we believe effective treatments need to be 3 dimensional too. Your brace will be designed using 3D full-body laser scanning technology, x-rays and posture photographs.
Each brace is then produced for the individual with Computer Aided design (CAD) and then created with Computer Aided Manufacture (CAM).
ScoliBrace is typically recommended for the treatment of Cobb angles from 25-50 degrees. It is suitable for wearers of all ages and comes custom-designed for your specific requirements. For curves less than 25 degrees, bracing may still be the preferred choice, as it’s a faster treatment than exercise – it’s also much easier for smaller children to manage (just put the brace on, rather than performing complex exercises). For curves greater than 50 degrees, bracing may still be possible – book an appointment with a scoliosis professional today!
Don’t forget that the UK Scoliosis clinic now offers online consultations too – so if you have questions, book an appointment today!
Images in this article are courtesy and copyright ScoliCare Australia.
[1] Dr Jeb McAviney, Superior In-brace Correction Achieved with a ScoliBrace Compared with a Standard TLSO in a Juvenile Scoliosis Patient (ScoliCare, 2020)

