Last week we began to explore the case of Patient X – a scoliosis patient who, after successful treatment with a ScoliBrace, avoided the need for corrective surgery and now lives scoliosis free. This week, we learn about her treatment prescription. If you missed week one, we suggest reading it here first.
3. The best treatment?
Having confirmed a scoliosis case and with that case being below the surgical threshold, it was possible to move forward with a non-surgical approach for patient x – but which is the best treatment methodology on offer?
In dealing with any scoliosis case, there are at least three elements to treatment which need to be considered – firstly, the Cobb angle (that is to say, the angle of the scoliotic curvature) needs to be reduced. Secondly the angle of trunk rotation (rib hump) and thirdly, muscular imbalances which have developed alongside the scoliosis, need to be addressed and balanced.
In terms of Cobb angle reduction, Scoliosis braces are the most effective non-surgical approach.[1] There are many different kinds of scoliosis brace and many work slightly differently. Broadly speaking braces can be classified as either active correction braces (which aim to reduce scoliosis by guiding the spine back to correct posture) and passive braces (which aim to prevent scoliosis from developing any further by holding the spine in its current position). Passive braces which are typically provided by hospitals, once the only option available, obviously do nothing to reduce cobb angle – so bracing with an active correction brace is the recommended approach.
The angle of trunk rotation or the “rib hump” is best addressed by a active scoliosis brace such as Scolibrace which addresses the scoliosis in a 3-dimensional manner, helping to de-rotate the spine to reduce rib hump progression, whilst preserving the spines natural curves in the low and mid-back.
The best approach to correcting the muscular and postural imbalances associated with scoliosis are specialised exercise methodologies which have been designed for scoliosis treatment. There are two main approaches to consider. The first is SEAS or the “Scientific Exercise Approach to Scoliosis”. SEAS consists of an individualised exercise program adapted for the purpose of treating an individual’s scoliosis. Different exercises are used to correct different types and elements of scoliosis, so by combining them in the correct way, an ideal exercise plan can be produced.
SEAS treatment is often used as a stand-alone approach when treating smaller curves and as a compliment to bracing with large curves and where there is a significant risk of progression.
The other main exercised based method, Schroth therapy, is a well-established and easy to use treatment methodology which some experts consider to be the best exercise-based approach for treating Idiopathic Scoliosis.[2] As an independent treatment, some studies have shown a reduction of Cobb angle of 10-15 degrees over the course of a year[3] – however, Schroth therapy combines particularly well with bracing. When Schroth is combined with bracing superior results can often be achieved more quickly than either approach alone.[4]
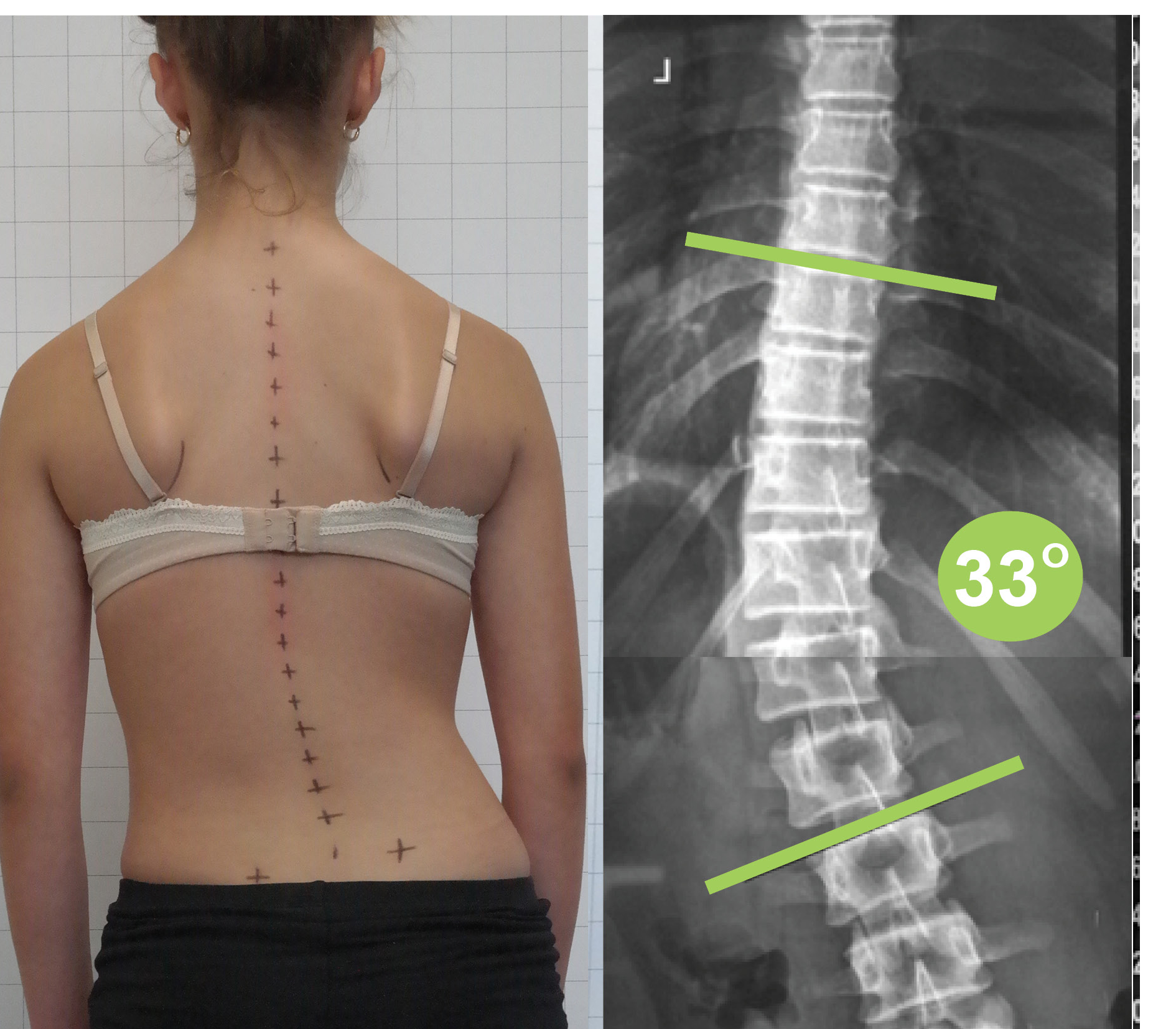
Patient x’s scoliosis, being 33 degrees cobb, was already beyond the point where exercise alone would have been an ideal treatment. As the patient was still growing and the curve was already greater than 30 degrees, she was also considered a high risk for her scoliosis to worsen. While this specific combination of factors meant that hers was a high-risk case overall, she was an ideal candidate for correction with a highly advanced scoliosis brace – the ScoliBrace. (This is the brace we offer at the UK Scoliosis Clinic)
In this case, scoliosis specific rehabilitation exercises and use of a scoliosis orthotic device, a Scolibrace, were therefore recommended.
4. Treatment with ScoliBrace
ScoliBrace, unlike many braces, is a totally customised, 3D designed, rigid active correction brace. ScoliBrace isn’t just customised for your scoliosis case, you can also choose a colour or pattern which suits your style – or opt for something which matches your skin tone to blend in well.
A ScoliBrace is not like most braces which use 3 point pressure. It uses a 3D inverse correction of the spine ie it shifts the spine into the opposite direction by moving the spine towards the correct position
For Patient X, the scoliosis brace was initially to be worn full-time. This is 23 hours per day with up to a maximum of 4 hours out of the brace if the patient was actively participating in sports during those out of brace hours. Brace wear was started at 2 hours on the first day, followed by adding another 2 hours every subsequent day until the required full-time hours were attained. Time in brace is often adjusted throughout scoliosis treatment period -but is generally high at the start in order to arrest the curve development and begin to reduce it as soon as possible.
Patient X was also given a program of scoliosis specific exercises, which were initially taught in the clinic as twice a week for 3 weeks, followed by once per month. The patient was required to complete the exercises each day out of the brace, but this was easy to do at home and it was included as brace time wear. A ScoliRoll (scoliosis orthotic device) was also used daily for 20 minutes to stretch the spine into the opposite direction of the curve, to help improve the spines mobility back to a normal position.
Next week, we’ll focus on Patient X’s progress with ScoliBrace!
[1] Yu Zheng, MD PhD et al. Whether orthotic management and exercise are equally effective to the patients with adolescent idiopathic scoliosis in Mainland China? – A randomized controlled trial study SPINE: An International Journal for the study of the spine (2018) [Publish Ahead of Print]
[2] Steffan K, Physical therapy for idiopathic scoliosis, Der Orthopäde, 44: 852-858; (2015)
[3] Kuru T, et al. The efficacy of three-dimensional Schroth exercises in adolescent idiopathic scoliosis: A randomised controlled clinical trial, Clinical Rehabilitation, 30(108); (2015)
[4] Marinela, Rață;Bogdan, Antohe, Efficiency of the Schroth and Vojta Therapies in Adolescents with Idiopathic Scoliosis. Gymnasium, Scientific Journal of Education, Sports, and Health Vol. XVIII, Issue 1/2017