When you or a loved one are first diagnosed with scoliosis its natural for your first thoughts to be about the best treatment available – and perhaps whether treatment is even necessary. Indeed, many medical professionals today still believe that a “wait and see” approach is the best way forward in most scoliosis cases. Despite this view, research is clear – scoliosis almost never resolves on its own whereas proactive treatment carries a very high success rate. Left untreated, scoliosis can be a life limiting condition, whereas the majority of patients treated with non-surgical methods today can live a totally normal life and often experience total curve correction.
What’s wrong with wait and see?

“Wait and see” is never the best approach
The “wait and see” approach (often called observation) means simply watching and waiting to see if a scoliosis case gets worse. This approach is based upon the (now outdated) view that surgery is the only effective option for scoliosis treatment. If your doctor or medical professional has recommended “wait and see” this does not mean they are being negligent however – historically surgery was thought to be the only effective treatment for scoliosis but today there are a wide variety of effective non-surgical options.
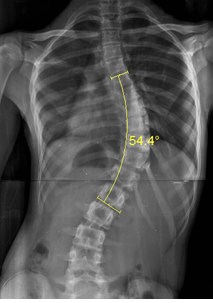
Non-surgical treatment for scoliosis has been shown to be successful up to 60 degrees cobb angle (cobb angle is the measure of scoliosis curvature), but the best results can be achieved when scoliosis is treated early. Since the objective of observation is simply to see if the scoliosis progresses to a significant enough curve to require surgery (typically 40 degrees plus) patients are often told to simply keep “waiting and watching” while their opportunity to maximise non-surgical approaches sadly slips away.
It can not be stressed enough that if you have been diagnosed with scoliosis and have been advised to “wait and see” you should contact a scoliosis clinic and schedule a consultation as soon as possible.
What happens if scoliosis is left untreated?
If scoliosis is left untreated, or a policy of “observation” is employed, scoliosis is overwhelmingly likely to continue to progress. In the very small number of cases where scoliosis does not progress it will certainly not reduce – meaning that (at best) the patient spends the rest of their life with symptoms associated with scoliosis.
Research has demonstrated that cases of Juvenile scoliosis greater than 30 degrees tend to progress quickly – studies suggest that 100% of these patients will progress to the surgical threshold. Juveniles with curves from 21 to 30 degrees are more difficult to predict in terms of progression but can frequently end up requiring surgery, or at least are left living with significant disability.[1]
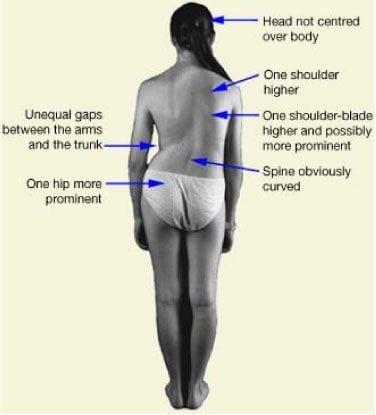
In cases which do not progress to the surgical threshold there are still many common symptoms which scoliosis sufferers will experience throughout their life without treatment. Some of the most common include pain, physical deformity, limited mobility and difficulty breathing during exercise.[2] Some recent research has also suggested that even a small cobb angle can have a significant negative impact upon a person’s ability to be active and keep fit and healthy.[3] Since we understand how important staying fit and active is to long term health, it is also fair to say that left untreated scoliosis could be a predictor for longer term health problems.
How can scoliosis be treated?
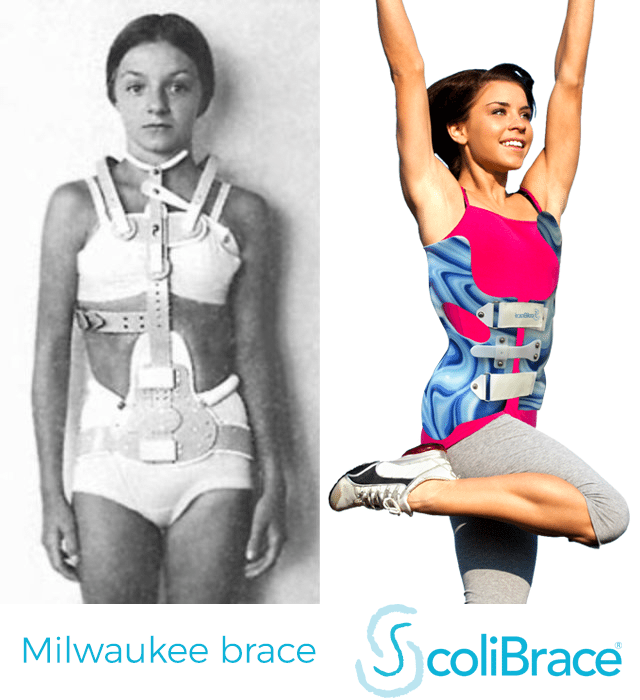
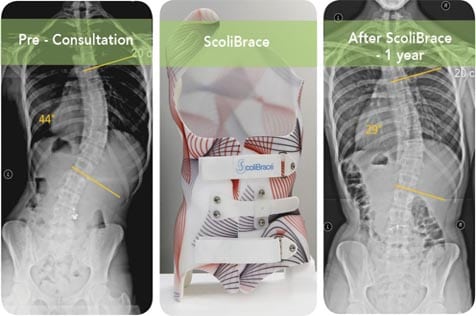
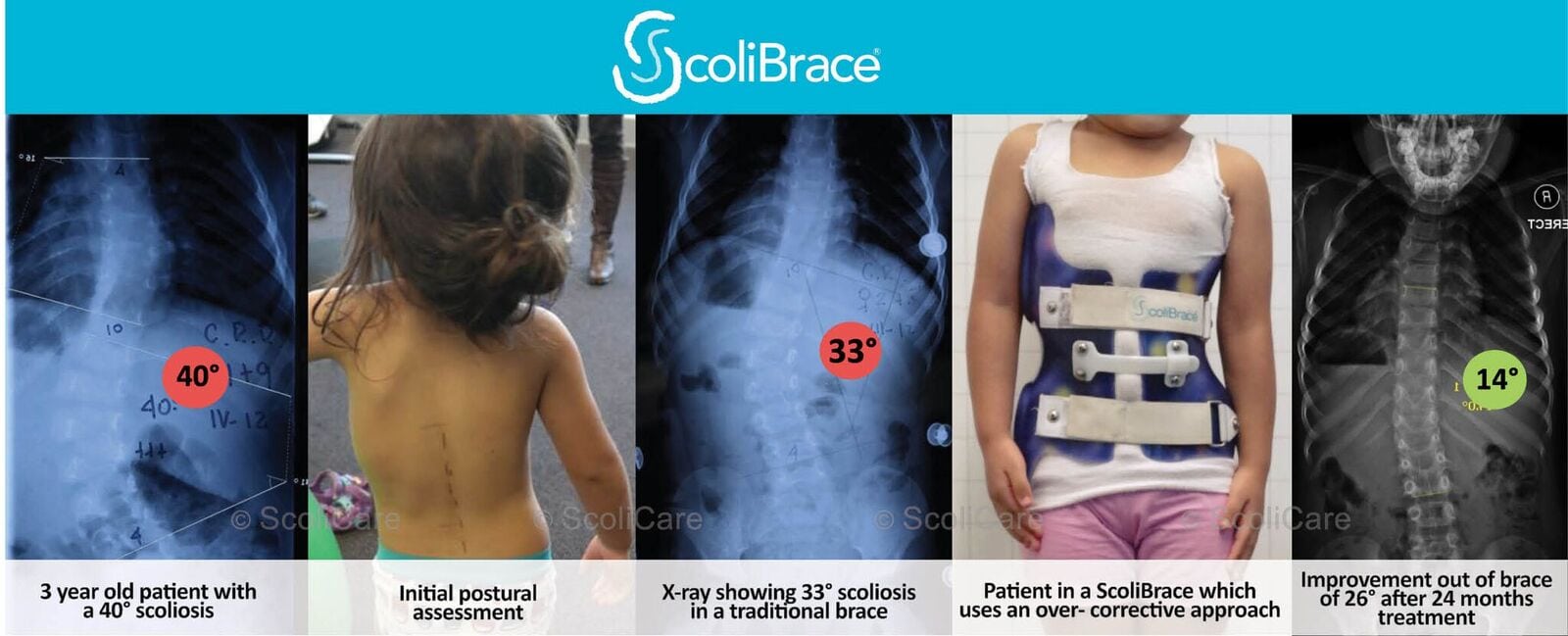
Today (while surgery remains and option for severe cases) most scoliosis patients can be treated non-surgically, although the sooner treatment is sought the better the prognosis and the simpler the treatment program required. Whereas “wait and see” can result in as much as 100% of patients progressing to the surgical threshold, through modern bracing technology it has been demonstrated that conservative treatment with a brace can reduce the number of patients requiring surgery to as low as 4.9% – in addition the vast majority of patients can active complete curve correction.[4]
[1] Progression risk of idiopathic juvenile scoliosis during pubertal growth, Charles YP, Daures JP, de Rosa V, Diméglio A. Spine 2006 Aug 1;31(17):1933-42.
[2] Sperandio EF, Alexandre AS, Yi LC, et al. Functional aerobic exercise capacity limitation in adolescent idio- pathic scoliosis. Spine J. 2014;14(10):2366–72. PubMed doi:10.1016/j.spinee.2014.01.041
[3] SARAIVA, BA; et al. “Impact of Scoliosis Severity on Functional Capacity in Patients With Adolescent Idiopathic Scoliosis”. Pediatric Exercise Science. 30, 2, 243-250, May 2018
[4] ‘Brace treatment in juvenile idiopathic scoliosis: a prospective study in accordance with the SRS criteria for bracing studies – SOSORT award 2013 winner‘ Angelo G Aulisa, Vincenzo Guzzanti, Emanuele Marzetti,Marco Giordano, Francesco Falciglia and Lorenzo Aulisa, Scoliosis 2014 9:3 DOI: 10.1186/1748-7161-9-3