Scoliosis is a condition that affects the curvature of the spine. It can be caused by a variety of factors, including genetics, injury, or underlying medical conditions. Scoliosis can range from mild to severe, and treatment options depend on the severity of the curvature. One of the most common treatments for scoliosis is bracing. While bracing can be effective in preventing further curvature of the spine, compliance with the treatment plan is crucial for success.
What is scoliosis bracing?
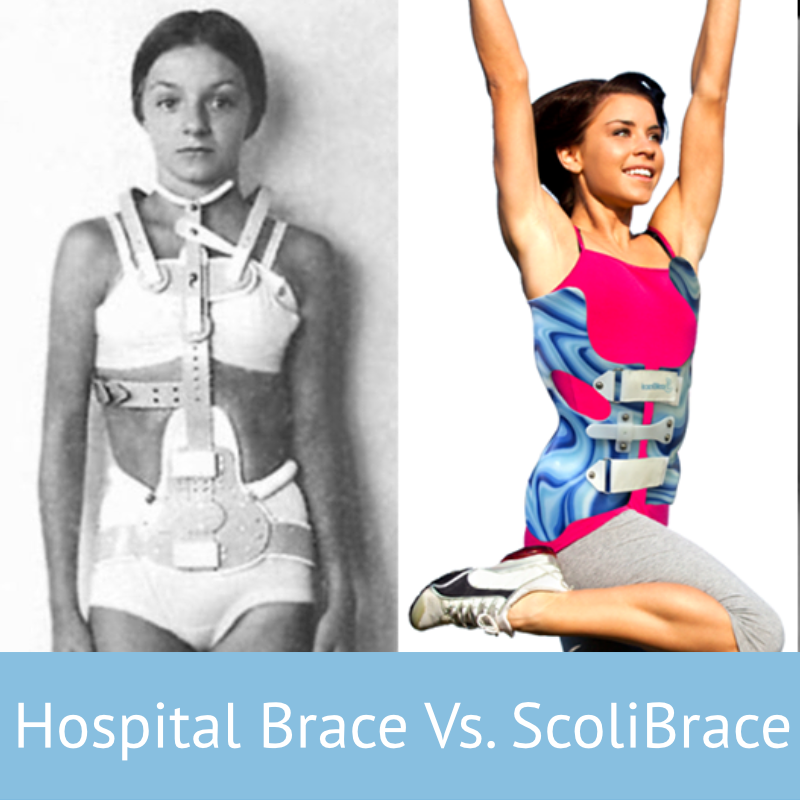
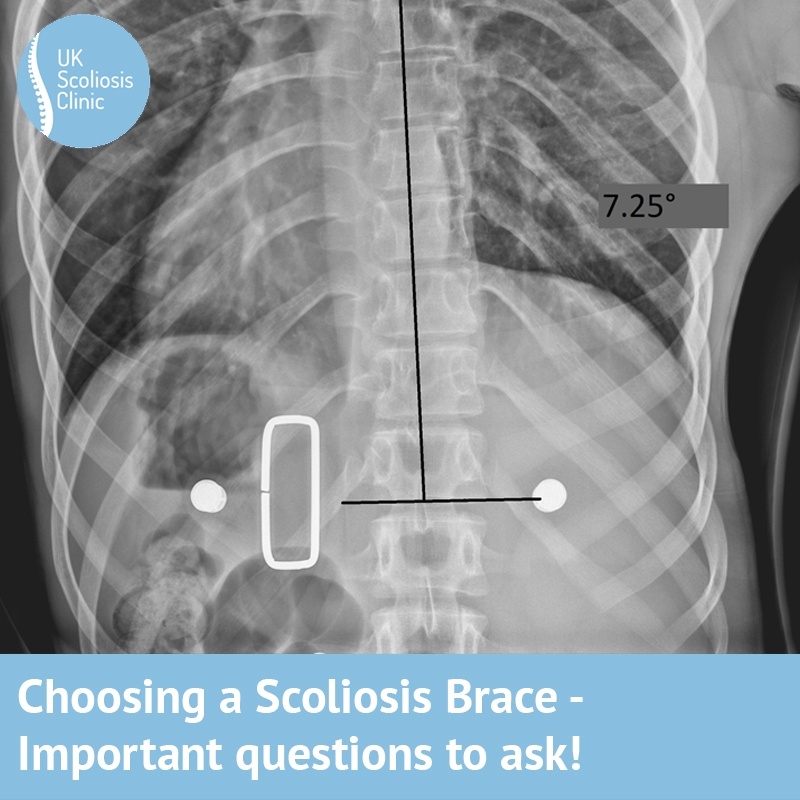
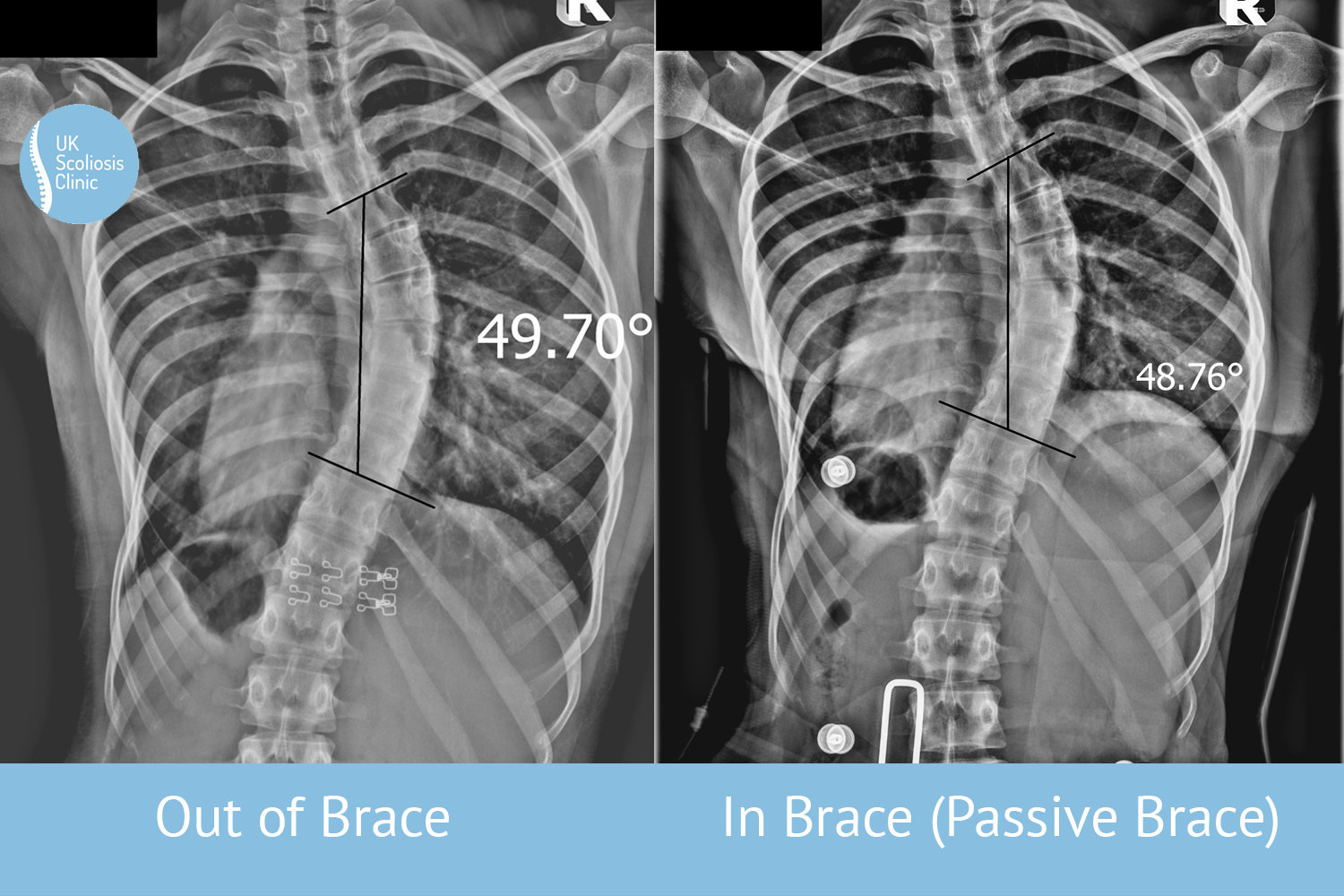
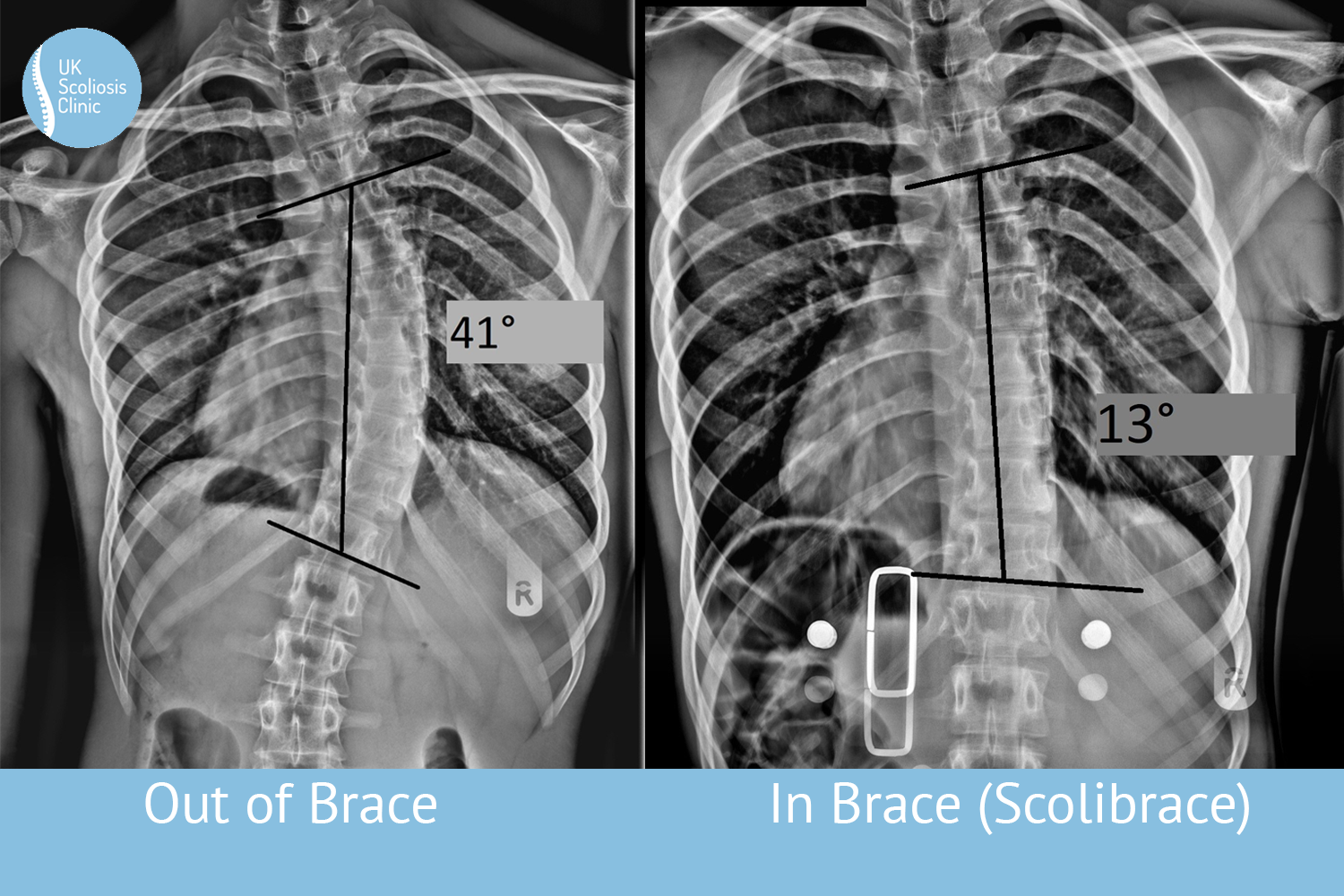
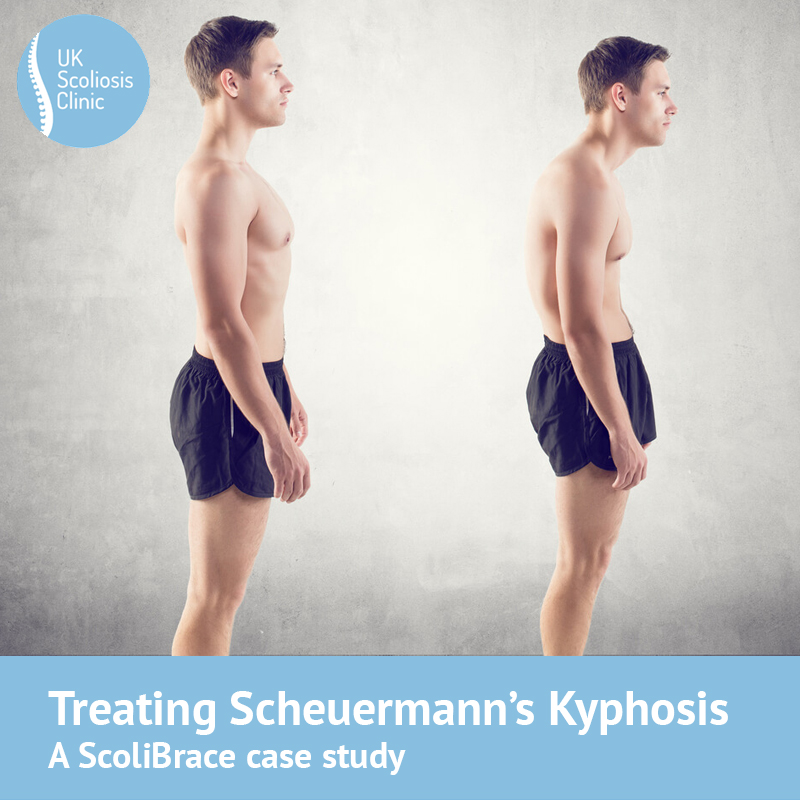
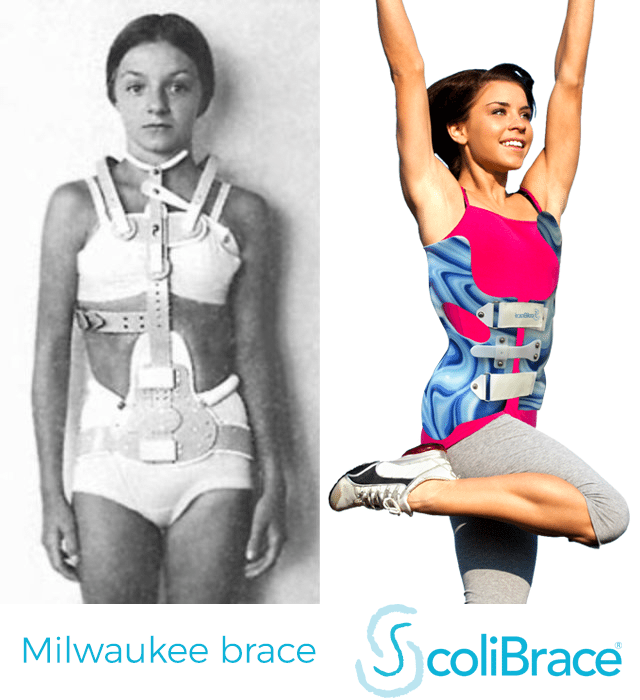
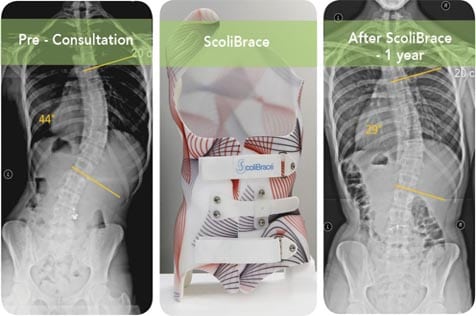
Scoliosis bracing involves the use of a custom-fitted brace to prevent further curvature of the spine. The brace is typically worn for a set number of hours each day, depending on the severity of the condition. The goal of bracing is to prevent further curvature and ideally, to reduce the existing curve. Modern “over-corrective” braces, such as the SoliBrace make this possible, whereas with older braces stopping progression was the best possible outcome.
Why is compliance important for scoliosis bracing success?
Compliance is crucial for the success of scoliosis bracing. When a patient wears a brace as directed by a Scoliosis specialist, they are more likely to prevent further curvature of the spine and reduce an existing curve. Compliance also ensures that the brace is working properly and providing the necessary support to the spine. Ultimately, Scoliosis braces work by gently applying pressure to the spine in a direction which opposes the curvature – over time, the spine will tend to correct itself – but time is the keyword here. Unless the brace is on a patient’s body for enough time, it simply cannot do its job.
Non-compliance, or failure to follow the treatment plan, can lead to a number of issues. If the patient does not wear the brace as directed, the spine may continue to curve, which can lead to more severe scoliosis and potential surgery. Non-compliance can also cause discomfort and pain, as the brace may not fit properly or provide the necessary support if the curve worsens from its “starting” state.
Compliance is therefore critical to the success of bracing – and while many patients often perceive this as a negative (especially when adjusting to brace wearing) it’s important to realise that research suggests this relationship is proportional, so, consider the flip side – the longer you wear the brace, the faster your Scoliosis will improve![1]
How can patients increase compliance with scoliosis bracing?
There are several strategies that patients can use to increase compliance with scoliosis bracing. The first step is to understand the importance of compliance and the potential consequences of non-compliance. Patients should of course discuss any concerns or questions they have with their specialist to ensure that they fully understand the treatment plan and have made as many adjustments as possible to make it viable – this is all well and good for adults but for children, it can be more complicated.
Parents of children being treated with Scoliosis braces should do everything they can to explain the process to their children, but on a practical level, they can also work to make the brace more comfortable and convenient to wear. This may involve adjusting the fit of the brace or finding ways to wear it that are more comfortable. Braces such as ScoliBrace are highly customisable and provide a lot of flexibility in this regard. Some patients find that wearing the brace while sleeping or during sedentary activities is more comfortable than wearing it during more active times – again, braces such as ScoliBrace are easy to put on or take off yourself, which makes it much easier to be more flexible with the times of day that a brace if worn.
Support from family and friends can also be helpful in increasing compliance. Encouragement and reminders to wear the brace can help patients stay on track with their treatment plan.
Is compliance the most important factor?
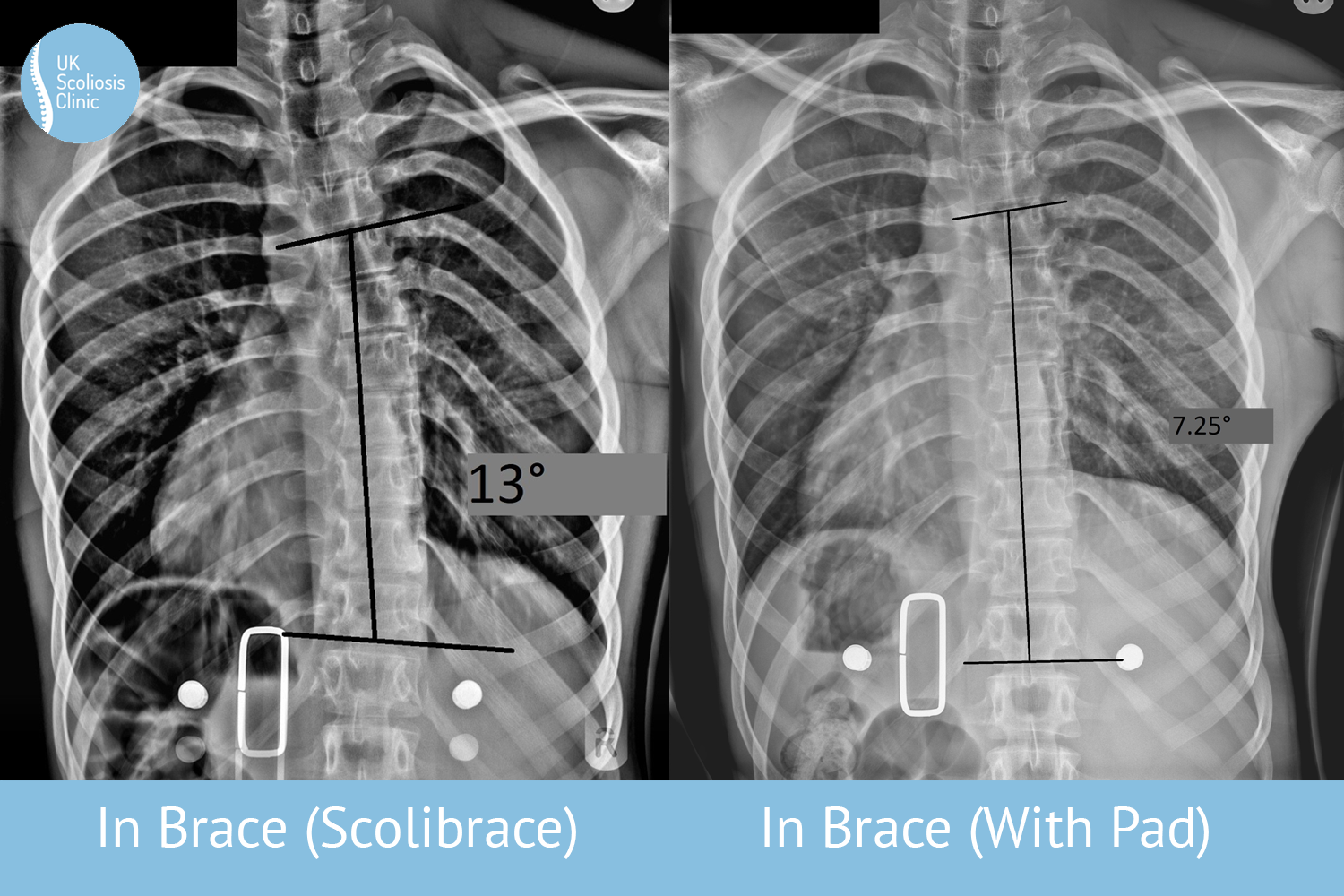
Compliance is crucial for the success of scoliosis bracing. When a patient wears a brace as directed, they are more likely to prevent further curvature of the spine and potentially improve a curve or at least avoid surgery. Nonetheless, compliance with a program is only valuable if that program is optimised to achieve individual results for a given patient – and this is why the choice of brace, and clinic matters so much.
[1] ‘Effects of Bracing in Adolescents with Idiopathic Scoliosis’
Stuart L. Weinstein, Lori A. Dolan, James G. Wright, and Matthew B. Dobbs, N Engl J Med 2013; 369:1512-1521 October 17, 2013DOI: 10.1056/NEJMoa1307337