Leg length discrepancy, commonly known as a short leg, and medically known as Anisomelia is a condition in which one leg is shorter than the other, resulting in a limping gait and often chronic lower back pain. In fact, a small leg length discrepancy is not unusual and is frequently treated by specialists such as a chiropractor – however, Anisomelia is said to occur if there is a difference of over 1cm, and surgery can be necessary for differences over 2cm.[1]
A short leg can cause scoliosis
Leg length discrepancy (LLD) has been observed in between 3–15% of the population[2] and there are two possible types, apparent or true.
True LLD is where the shortening of one leg compared to the other can lead to scoliosis as the body tries to compensate. In this case, scoliosis will usually reduce when the LLD is treated.
By contrast, apparent LLD is a symptom of a problem, not the actual cause. Apparent LLD is a condition in which the legs are actually the same length but appear to be different due to an underlying pelvic or spine disorder. In this case, treating the pelvic and/or spine disorder resolves the LLD.
Because of these relationships, it has long been suggested that True LLD can cause or worsen scoliosis[3] – despite this, there had not been any definitive studies on the relationship between LLD and scoliosis until this year.
How common is LLD in scoliosis patients?
Despite the fact that many health professionals see a link, information on the exact relationship of LLD to scoliosis has been difficult to obtain and studies have produced mixed results. One study of 23 young adults[4] suggested that scoliosis was minor in patients with discrepancies of < 2.2 cm. At the other end of the scale, another study measuring the x-rays of 106 patients in a private chiropractic practice showed that those with LLD > 6 mm often (53% of the cases) had scoliosis and/or abnormal lordotic curves.
Does LLD cause scoliosis?
There has certainly been evidence to suggest that there may be a causal link between LLD and scoliosis. Although a direct link has not been established, it Is accepted that LLD causes pelvic obliquity.[5] Pelvic obliquity simply means that one side of the pelvis sits higher than the other. Since we also know that 40% to 60% of children with lumbar scoliosis also have pelvic obliquity, it seems reasonable to suggest that LLD may indirectly lead to scoliosis.[6]
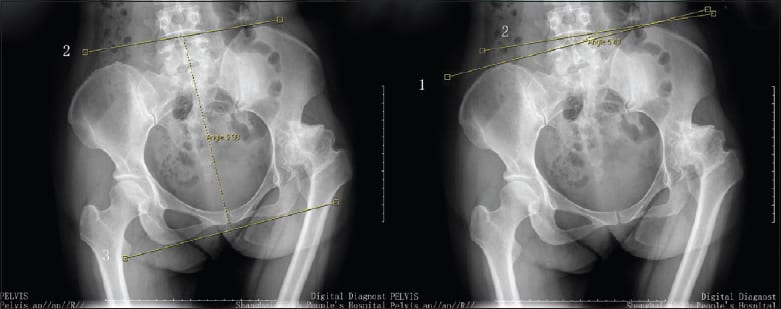
Pelvic Obliquity is common in scoliosis patients
LLD and Scoliosis, new research results
With this background in mind, a 2018 study[7] aimed to find out if there is a measurable association between pelvic obliquity, LLD and the scoliotic curve in an adolescent patient or not. The researchers also wanted to discover whether scoliotic curve progression was linked to different amounts of leg length discrepancy
During the study, seventy-three patients with an average age of 13.3 years at initial examination were given an X-Ray and then had this compared with a later follow up. Scoliosis was confirmed in all 73 patients. At initial examination, pelvic obliquity appeared in 23 (31.5%) patients with scoliosis, and LLD was identified in 6 (8.2%) patients with scoliosis and pelvic obliquity. The majority of the patients in the study were under observation for their scoliosis, allowing the researchers to observe the relationship between scoliosis and leg length.
At a subsequent visit, at an average of 2.8 years later, no significant change in LLD was observed, but a statistically significant increase in scoliotic and pelvic deformity was found. The study, therefore, concluded that in the adolescent patient population with thoracic or thoracolumbar scoliosis, the LLD remains stable with growth but both the scoliotic deformity and pelvic obliquity continue to progress.[8]
So what is the relationship between LLD and scoliosis?
This most recent study suggests that in adolescent patients at least, LLD stays stable and does not seem to have a direct association with the progression of scoliosis. Having said this, the small number (6 out of 73, 8.3%) of patients with LLD in this study suggests that a larger sample set should be explored before drawing any firm conclusions.
Perhaps most importantly, the authors suggest that future research could focus on younger patients less than 10 years with LLD to detect early-onset scoliosis prevalence and how it changes with growth and treatment since it is entirely possible that LLD may have a more significant impact at this early stage.
For now, it seems advisable to conclude that LLD is just one of a number of conditions which can be associated with scoliosis, and certainly with spinal disorders more widely. If you or a loved one have noticeable LLD, it is advisable to see a spinal specialist.
[1] Steen H, Terjesen T, Bjerkreim I, Anisomelia. Clinical consequences and treatment Tidsskr Nor Laegeforen. 1997 Apr 30;117(11):1595-600.
[2] Gurney B. Leg length discrepancy. Gait Posture. 2002;15:195–206.
[3] Steen H, Terjesen T, Bjerkreim I, Anisomelia. Clinical consequences and treatment Tidsskr Nor Laegeforen. 1997 Apr 30;117(11):1595-600.
[4] Papaioannou T, Stokes I, Kenwright J. Scoliosis associated with limb-length inequality. J Bone Joint Surg. 1982;64:59–62.
[5] Anderson M, Green WT, Messner MB. Growth and predictions of growth in the lower extremities. J Bone Joint Surg. 1963;45-A:1–14.
Asher MA. Scoliosis evaluation. Ortho Clin North Am. 1988;19:805–14.
Brady RJ, Dean JB, Skinner TM, Gross MT. Limb length inequality: clinical implications for assessment and intervention. J Orthop Sports Phys Ther. 2003;33:221–34.
Burwell RG, Aujla RK, Freeman BJ, Dangerfield PH, Cole AA, Kirby AS, et al. Patterns of extra-spinal left-right skeletal asymmetries in adolescent girls with lower spine scoliosis: relative lengthening of the ilium on the curve concavity & of right lower limb segments. Stud Health Technol Inform. 2006;123:57–65.
Cummings G, Scholz JP, Barnes K. The effect of imposed leg length difference on pelvic bone symmetry. Spine. 1993;18:368–73.
D’Amico M. Scoliosis and leg asymmetries: a reliable approach to assess wedge solutions efficacy. Stud Health Technol Inform. 2002;88:285–9.
[6] Schwender JD, Denis F. Coronal plane imbalance in adolescent idiopathic scoliosis with left lumbar curves exceeding 40 degrees: the role of the lumbosacral hemicurve. Spine. 2000;25:2358–63.
Walker AP, Dickson RA. School screening and pelvic tilt scoliosis. Lancet. 1984;2:152–3.
[7] Avraam Ploumis et al. Progression of idiopathic thoracic or thoracolumbar scoliosis and pelvic obliquity in adolescent patients with and without limb length discrepancy Scoliosis and Spinal Disorders 2018 13:18
[8] Specht DL, De Boer KF. Anatomical leg length inequality, scoliosis and lordotic curve in unselected clinic patients. J Manip Physiol Ther. 1991;14:368–75.
