For some time now, scoliosis clinicians have broadly accepted the view that scoliosis bracing is an effective way to halt the progression of scoliosis, and (with the use of the correct brace) is also an effective way to reduce the curve.
The outlook for bracing was not always a positive as it is today – historically, studies suggested that bracing was only as effective as observation. Over time however, research has tended to show bracing to be more effective than was once thought, so that today the rates of success with bracing are very high.
In 2005, the Scoliosis Research Society (SRS) attempted to standardize the inclusion criteria and outcome measurements for bracing studies, to enable comparison among studies. In the guidelines, it was suggested that a curve progression of less than 5 degrees should be regarded as success. At the time, SRS did not even consider that bracing might actually serve to improve a curve – although it was quickly realised that this was possible. For this reason, the criteria for “improvement” (being a reduction of curve of at least 6 degrees) was established in 2009.
Despite some scepticism in the mid 2000’s however, some bracing studies today have demonstrated rates of surgery prevention as high as 100%[1][2] and the field is one of the major areas of study and advancement – so what caused such an improvement in the prognosis?
Braces are getting better
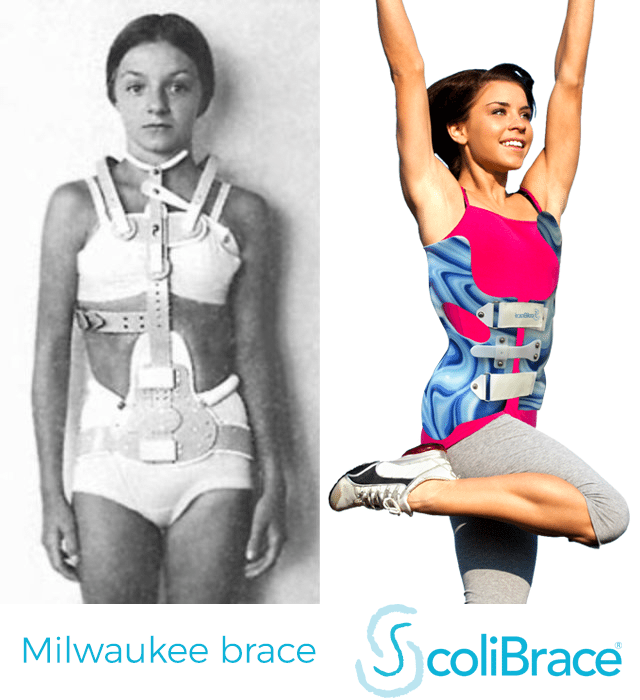
Scoliosis braces have come a long way!
One of the major reasons for the improvement in bracing effectiveness has been the improvement in braces themselves. A recent review study conducted in 2016, attempted to explore this issue by examining 53 studies published between 1990 and 2016[3]. It showed that when comparing the percentage of patients eventually requiring surgery and the improvement rate in the past 26 years, we find that there is a trend towards reduction in surgical rate and an increase in improvement rate. Yet, close inspection showed that the change is strongly related to the type of brace used.
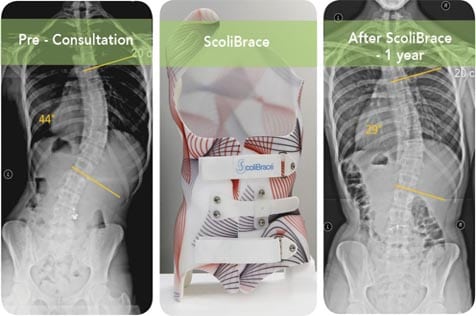
Key factors in bracing outcome are the amount of in-brace correction and comfort for the wearer. In the study, it was shown that large in-brace correction in excess of 50% would be accompanied by improvement at skeletal maturity[4][5] and hours of brace wear are positively associated with the rate of treatment success[6]. Simply put, an active correction brace which is also comfortable to wear is a key factor in significantly reducing surgical requirement[7]. This is why so much effort has been expended in ensuring that our ScoliBrace is the most comfortable brace available!
The study also showed that the effectiveness of a brace depended on the quality of its construction, not just its design[8]. In 2007 Danielsson et al pointed out the importance of the skill and dedication of the orthotist in creating a brace as a critical factor in the eventual success of treatment and similar views have been forwarded by other authors[9]. Today, advancements in technology mean that a higher quality of brace design and manufacture than ever before is available to us. Indeed, at the UK scoliosis clinic we use the latest laser scan and computer aided manufacture processes to create a brace for each client, which fits their needs perfectly.
Combination treatment is most effective
Today we also appreciate that in most instances an individualised treatment plan based on a number of complementary methods provides the best chance for a significant reduction of the curve. In fact, today it is generally accepted that bracing should not be employed alone in the management of Adolescent Idiopathic Scoliosis in particular – instead individualised scoliosis specific exercises should also be incorporated. This is because Scoliosis specific exercises improve the muscle strength of the trunk and the postural awareness of the patients. More importantly perhaps, when combined with bracing, evidence suggests the results are an improvement in curve reduction[10]. Properly tailored exercise programs may also help to reduce the loss of correction which frequently accompanies the end of brace treatment if not properly managed.[11]
Scoliosis clinicians are working hard to improve bracing technology.
Modern scoliosis braces are highly effective
At the UK scoliosis clinic, we respect and value the work that surgeons can do in correcting very serious cases of scoliosis which are unsuitable for conservative treatment. However, the 2016 review study has suggested that a conflict of interest in bracing development might be a negative factor for patients[12].
One of the lest effective forms of brace is the Boston brace – yet these are often favoured by orthopaedic surgeons (especially in the US)[13]. The Boston brace is at least outdated, and in some situations may complicate scoliosis treatment unnecessarily. Boston braces also encourage thoracic flat back, which has been shown to be detrimental to the correction of curves[14].
Why are these braces sometimes favoured then? – This maybe because in the event that the brace fails to achieve the objective, the surgeon can go on to treat the patient using surgery, although this might not be the patient’s preference. Conversely, the kinds of modern braces we use at our clinic and which are widely implemented throughout Europe today are predominantly used by physicians who treat patients conservatively. In this instance, failure of the brace requires an external referral for surgical treatment[15] – hence it is in the interest of non-surgical clinics to constantly develop and improve their braces, which results in highly advanced modern braces, like ScoliBrace.
[1] De Giorgi S, Piazzolla A, Tafuri S, Borracci C, Martucci A, De Giorgi G. Chêneau brace for adolescent idiopathic scoliosis: long-term results. Can it prevent surgery? Eur Spine J.2013;22(6):S815–22.
[2] Aulisa AG, Guzzanti V, Perisano C, Marzetti E, Falciglia F, Aulisa L.Treatment of lumbar curves in scoliotic adolescent females with progressive action short brace: a case series based on the Scoliosis Research Society Committee Criteria. Spine (Phila Pa 1976). 2012;37(13):E786-E791.
[3] Wing-Yan CHAN, Shu-Yan NG, Tsz-Ki HO, Yin-Ling NG (2016) Bracing – Halting Progression or Improving Curves in Adolescent Idiopathic Scoliosis. J Rheumatol Arthritic Dis 1(1): 1-8.
[4] Landauer F, Wimmer C, Behensky H. Estimating the final outcome of brace treatment for idiopathic thoracic scoliosis at 6-month follow-up.
[5] Appelgren G, Willner S. End Vertebra Angle – A roentgenographic method to describe a scoliosis. A follow-up study of idiopathic scoliosis treated with the Boston brace. Spine (Phila Pa 1976) 1990;15(2):71- 74.
[6] A large number of studies are cited in Wing-Yan CHAN, Shu-Yan NG, Tsz-Ki HO, Yin-Ling NG (2016) Bracing – Halting Progression or Improving Curves in Adolescent Idiopathic Scoliosis. J Rheumatol Arthritic Dis 1(1): 1-8.
[7] Wiley JW, Thomson JD, Mitchell TM, Smith BG, Banta JV. Effectiveness of the Boston brace in treatment of large curves adolescent idiopathic scoliosis. Spine. 2000;25(18):2326–2332.
[8] Rigo MD, Villagrasa M, Gallo. A specific scoliosis classification correlating with brace treatment: description and reliability. Scoliosis. 2010;5(1):1. doi:10.1186/1748-7161-5-1.
[9] For example see Rowe DE, Bernstein SM, Riddick MF, Adler F, Emans JB, Gardner- Bonneau D. Ameta-analysis of the efficacy of non-operative treatments for idiopathic scoliosis. J Bone Joint Surg Am. 1997;79(5):664-674.
[10] Monticone M, Ambrosini E, Cazzaniga D, Rocca B, Ferrante S. Active self-correctionand task-oriented exercises reduce spinal deformity and improve quality of life insubjects with mild adolescent idiopathic scoliosis. Results of a randomized controlled trial. Eur Spine J. 2014;23(6):1204-14. doi:10.1007/s00586-014-3241-y.
[11] Goldberg CJ, Dowling FE, Hall JE, Emans JB. A statistical comparison between natural history of idiopathic scoliosis and brace treatment in skeletally immature adolescent girls. Spine. 1993;18(7):902-9088.
[12] Wing-Yan CHAN, Shu-Yan NG, Tsz-Ki HO, Yin-Ling NG (2016) Bracing – Halting Progression or Improving Curves in Adolescent Idiopathic Scoliosis. J Rheumatol Arthritic Dis 1(1): 1-8.
[13] Wynne JH. The Boston brace and TriaC system. Disabil Rehabil Assist Technol2008; 3(3):130-135. doi:10.1080/17483100801903988.
[14] Wing-Yan CHAN, Shu-Yan NG, Tsz-Ki HO, Yin-Ling NG (2016) Bracing – Halting Progression or Improving Curves in Adolescent Idiopathic Scoliosis. J Rheumatol Arthritic Dis 1(1): 1-8.
[15] Ibid.
